
May 19, 2022

Overcoming Medical Orthodoxy (Part 4): Retooling Clinicians for “New Medicine”
Author Note: This is the final article in a four-part series on reinventing medical education and clinician training. Part 1 and Part 2 identify sources of dysfunction in medical education and solutions for addressing them. Part 3 identifies several powerful forces that are disrupting established medical practices and paving the way for “New Medicine’s” emergence. This article explores strategies for enhancing clinicians’ capabilities to practice value-based care and population health medicine.
In 2007, Donald Berwick and his colleagues at the Institute for Healthcare Improvement introduced the concept of healthcare’s Triple Aim. In Berwick’s words, “Improving the U.S. health care system requires simultaneous pursuit of three aims: improving the experience of care, improving the health of populations, and reducing per capita costs of health care.”
Since then, many have argued that “improving the work life of health care providers, including clinicians and staff” should become the fourth aim. More recently, some have argued that “health equity” should become the fifth aim.
Together, these five aims are the foundation of New Medicine and contrary to well-established Old Medicine practices. Achieving this “Quintuple Aim” requires clinical practice models that emphasize interdisciplinary as well as interprofessional team-based care, human-machine collaboration and lifelong learning.
Innovative medical schools are making notable strides in advancing these quintuple aims, but “Old Medicine” still dominates in most hospitals and clinics across the country. Old Medicine’s greatest failure is its unwillingness to embrace team-based care models where all clinicians practice in concert at top-of-license to drive better care outcomes and patient experience.
Management guru Peter Drucker observed, “If you want to do something new, you have to stop doing something old.” For medicine, that requires clinicians to unlearn Old Medicine’s entrenched and counterproductive practices while embracing New Medicine’s data-driven and customer-centric models for care delivery.
Retooling America’s clinical workforce to practice New Medicine is an enormous undertaking. No initiative of this scope occurs in a vacuum. Across all industry sectors, companies are adapting to remarkable advances in digital technologies and analytics. Healthcare is no exception. Harnessing digital technology’s potential is a team-based enterprise. Clinical training and leadership development must evolve to create healthcare’s workforce for tomorrow.
Old Medicine vs. New Medicine
Old Medicine applies a heroic model of physician leadership that discourages team-oriented behaviors. Reflective of a time when most physicians worked independently, such an approach grants enormous autonomy to physicians but impedes standardization, compromises patient safety and diminishes care outcomes.
New Medicine relies on continuous performance improvement supported by massive data sets and incisive analytics. Integrated technologies improve medical decision-making at the point of care. Optimizing performance requires ongoing clinical education that is relevant, seamless and connected to operational workflows. It must facilitate learning without adding more administrative burden to already overworked clinicians.
Unfortunately, most Continuing Medical Education (CME) curriculum adheres to Old Medicine’s leadership dynamics and cultural preferences. This chart contrasts Old Medicine’s learned behaviors with those required to excel within New Medicine’s evolving ecosystem.
In New Medicine, collaborative, team-based leaders engender trust and share information freely. They replace command-and-control leaders who practice hierarchical decision-making and cherish individual autonomy. Outcomes improve as dynamic teams prioritize patients’ needs, collaborate and hold one another accountable.
Human capital is New Medicine’s most precious resource. Leadership development tools and data support self-assessment, self-awareness and personal and professional growth. Coaching, training and guidance can equip physicians and other clinicians to control their emotions, become more empathetic and encourage patients to become active participants in their
care regimens.
Inculcating New Medicine’s aligned educational programming into daily work routines is a powerful tool for unifying organizational culture, enhancing capabilities, optimizing performance and realizing workforce potential. In this organic and systematic way, educational programming creates the principal channel for developing the essential learned leadership behaviors required for “new medicine” to thrive.
Reinventing Continuing Medical Education
A striking aspect of current CME practices is its outdated reliance on in-person or online classroom learning. This is a poor substitute for timely information and insights delivered through digital technologies within workflows.
For the first time ever, the rate of technological change is greater than human adaptability (see chart). This innovation-adaptation conundrum presents both a daunting challenge and remarkable opportunity for incumbent providers to develop high-performing workforces.
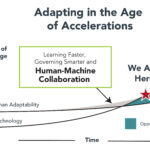
Source: Thank You for Being Late: An Optimist’s Guide to Thriving in the Age of Accelerations. Thomas L. Friedman, 2016.
Medical knowledge already far exceeds human capability to acquire and retain. CME credits perpetuate an unwinnable and exhausting knowledge chase. Human-machine collaboration optimizes human potential. Computer algorithms track, crunch and analyze voluminous amounts of data to offered individualized prompts at the point of care. This frees medical professionals make better-informed decisions and engage more effectively with patients.
Achieving New Medicine’s promise requires a different way of thinking about professional education and the workforce development. By reconfiguring and aligning its educational assets, healthcare organizations can enhance employee recruitment and retention, improve productivity, job satisfaction and performance, reduce burnout, increase profitability and create an engaged, empathetic and consumer-centric workplace culture.
In essence, provider organizations must become a source of lifelong learning for their healthcare professionals. Ongoing education cannot be ad hoc and disconnected from operations. It must be relevant and support continuous individual and organizational performance improvement.
As an industry, healthcare must move beyond certification programs to encompass broader simulation and virtual reality training, online courses, team-based training, coaching and experiential learning. From the beginning of a career to retirement, programs must teach, coach and cultivate core skills all clinicians need in the digitally enabled, highly complex, consumer-focused, collaborative and information-saturated care delivery environments. Clinicians need these core skills to deliver compassionate, effective and efficient care.
Enlightened organizations, including the Cleveland Clinic and Providence, are overhauling their approaches to professional training and education to create high-performing care teams.
Promising Provider Initiatives: Team of Teams Taking Hold
The Cleveland Clinic and Providence are very different types of health systems. The Clinic is a multi-specialty academic medical center with affiliated hospitals and centers around the world and a sterling reputation for scientific excellence and customer service. Providence is a massive, religiously-sponsored, community-focused healthcare provider in seven western states with annual revenues more than double the Clinic’s ($27.3 billion in 2021 versus $12.4 billion).
While different in orientation, the Clinic and Providence share a deep commitment to professional development, lifelong learning and team-based care delivery. They manifest this commitment through substantial investments in experiential learning, individualized programming and adaptive problem-solving. Each is building a “New Medicine” workforce that engages with patients, works collaboratively across professions and employs technology to optimize care outcomes and individual wellbeing.
Launched in 2020, the Clinic’s Mandel Global Leadership and Learning Institute trains physicians, administrators, nurses and other caregivers under one roof to become the strategic and conceptual thinkers needed to lead healthcare’s future. Kelly Hancock is the Clinic’s first Chief Caregiver Officer. Hancock, who oversees professional development for the Clinic’s 70,000 caregivers, describes their approach to cultivating team-based leaders as follows,
“To be successful in the future, we must change the way we enculturate, train and develop leaders…We apply all available tools and resources not only to aid leaders in their personal growth, but even more importantly, to develop together as teams.”
The Institute’s mandate supports the way clinicians learn to practice care. All Clinic professionals meet in team huddles every day at the same time to review the prior day’s events in relationship to the organization’s four care priorities: patients; caregivers, organization and community. The input from the team huddles cascades up through the Clinic’s six leadership tiers and shapes real-time organizational learning and responsiveness. Hancock believes that overcoming silos and embracing a team-of-teams culture is the secret ingredient that will keep the Cleveland Clinic among world’s leading healthcare providers.
With a similar commitment to lifelong learning and team-based care, Providence launched its Clinical Academy in 2015 within its Nursing Institute to provide new graduate nurses with a foundation for long-term professional success. The Academy has been remarkably effective at improving morale, reducing turnover, enhancing quality and lessening burnout. Since its launch, the Academy has trained over 14,000 nurses, cut turnover among its cohorts by more than 50% and saved Providence in excess of $150 million.
Nurses participate in a one-year initial training program and return in year two or three to train in one of 22 clinical specialties. According to LeAnn Ogilvie, the Academy’s Executive Director, the program’s “secret sauce” is treating participants “the way we all want to be treated.” The curriculum includes interactive learning with an emphasis on real-world simulation, a preceptor program that pairs new nurses with senior colleagues for the first 12-28 weeks (depending on specialty) and robust competency-based learning.
Operating across a broad geography with 52 hospitals and over a thousand clinics, Ogilvie sees real benefit in the Academy’s support for a “One Providence” operating culture that enhances team-based care delivery, minimizes errors and emphasizes patient engagement. As she notes,
“Having more nurses with Academy training reduces the operational variation between Providence’s hospitals and clinics. It’s not as big a leap to transfer to another Providence facility in another state as it is to go to an entirely new facility. Quality improves too as the Academy’s advanced clinical content and practices take root through our graduates. The whole ecosystem flourishes.”
High-functioning teams with individuals practicing at top-of-license are the essence of New Medicine’s superior care delivery model. As both the Cleveland Clinic and Providence approaches illustrate, team-based care doesn’t occur by chance. It requires intentional investment in innovative and well-designed training programs to sustain lifelong learning and continuous performance improvement.
Charting a Course
Like the Cleveland Clinic and Providence, health systems can leverage their investments in educational programming to promote value-based care delivery and population health business practices organically. Specifically, a reconfigured educational program could do the following to facilitate high-value holistic care delivery, promote risk-based business models and accommodate consumerism:
- Expand digital curriculum.
- Advance experiential learning.
- Promote interdisciplinary and interprofessional service delivery.
- Align high performing management and leadership capabilities.
- Promote adaptive behaviors and mobility.
- Establish a culture of feedback, self-assessment and lifelong learning.
- Create status related to completing management and leadership programs.
The ancient Chinese proverb applies, “A journey of a thousand miles starts with a single step.” Transforming a medical delivery culture steeped in tradition and wedded to fee-for-service payment will not be easy nor happen overnight.
The amount spent annually on CME constitutes a trivial percentage of the nation’s annual $4 trillion healthcare expenditure. Properly directed, however, CME programming can become a meaningful force for promoting New Medicine behaviors and building a stronger healthcare workforce.
Success requires centralizing and systematizing the administration of educational programs within the health system. Professional training must encompass a common set of “action skills” that includes communication, collaboration, understanding of roles and responsibilities, critical thinking, empathy, active listening, asking questions, and observational skills. More advanced professionals must become experts in advocacy, conflict resolution and change management.
Educational programming with interprofessional and interdisciplinary teams will emphasize experiential learning to provide context, real-world training and insight. Virtual space is real space. Like airline crews, healthcare professionals will hone their skills through simulation exercises that push responsibility to individuals on the front lines supported with real-time data and immediate feedback.
Effective communications will be more essential than ever. Incorporating unique learning techniques such as improvisation and storytelling, will build agile and adaptive leaders/managers who use persuasion to achieve desired results. Expanded professional development will incorporate lifelong learning to build new skills and enable enhanced collaboration among humans and with machines.
To propel forward, healthcare organizations must develop a unified vision for educational programming that can shape tactical decisions across the entire care continuum. The “parts’’ must contribute to a greater whole. With an articulated and aligned end-in-mind, decision-makers can create a roadmap to guide in reconfiguring its CME programming. That roadmap could include the following components:
- Consider granting visible recognition to individuals and teams that complete training – make employees eager to receive training.
- Incentivize lifelong learning as both an individual and corporate responsibility.
- Emphasize team-based experiential learning, delivered with context, to foster interdisciplinary and interprofessional collaboration and alignment.
- Create a core curriculum for all clinicians that incorporates organizational learnings (e.g., history, values and mission) and develops “action” skills (communication, listening, empathy, synthesis, adaptability, etc.) that enhance professional performance.
- Evaluate and recruit program candidates and new employees that have desired characteristics (e.g., appropriate technical competencies) and advanced “action” skills
- Build on existing program successes to win wider organizational support
- Purposefully recognize training that employees receive, like becoming proficient operating new equipment, through their daily work.
- Intentionally structure learning opportunities, where possible, within an employee’s workday. Digital and virtual technologies make it possible to teach, learn, and track education programming more easily.
In a compounding manner, these types of initiatives create momentum for constructive organizational change that advances value-based care delivery and population health management. Effective educational programming develops and sustains high-performing professionals.
Conclusion: The Urgency of Now
Helen Keller observed, “The only thing worse than being blind is having sight but no vision.” Old Medicine, addicted to FFS payment, is lumbering into an uncertain future with a voracious appetite for resources but no vision for transforming itself.
A new world order is emerging within medicine that is shaking Old Medicine’s foundations to the core. Revolutionary New Medicine centers on meeting consumer’s needs, creating value, emphasizing well-being and using technology to improve outcomes and convenience.
 Orthodoxies rarely concede without a fight, but they can adapt and remain relevant. Incumbent providers cannot afford to waste resources on ineffective education and training programs. They can participate in New Medicine’s reformation, but it will require massive cultural and organizational change. Reinventing CME to retool healthcare professionals, most-notably physicians, is prerequisite for success.
Orthodoxies rarely concede without a fight, but they can adapt and remain relevant. Incumbent providers cannot afford to waste resources on ineffective education and training programs. They can participate in New Medicine’s reformation, but it will require massive cultural and organizational change. Reinventing CME to retool healthcare professionals, most-notably physicians, is prerequisite for success.
The future belongs to team-based, consumer-oriented health companies that delivery high-value services consistently and with a smile. Not known for their agility, health systems must exhibit the flexibility and adaptability required to sustain market relevance within the disrupting healthcare marketplace.
Acknowledging the need for change is an important first step, but it cannot stop there. Health systems must develop and administer incisive training and development programs to create New Medicine’s workforce of the future. Team of teams operating cultures will be the secret ingredient that can transform healthcare delivery.
Healthcare’s greatest resource is its people. Teach them well and let them lead the way.
Read All 4 parts of this series on Overcoming Medical Orthodoxy

About the Authors
Recent Posts


