
April 24, 2019
Let’s Get Real: Medicare for All Can’t Work, but Affordable Health Insurance for All Can
As it has in the last three presidential elections, healthcare is emerging as a decisive political issue in the 2020 election. Unlike in those previous elections, however, universal health insurance in the form of “Medicare for All” (M4A) is taking center stage in the political debate.

Most notably, Democratic front-runner Senator Bernie Sanders outlined has proposed a very generous M4A plan that would phase out commercial health insurance over four years and include long-term care, vision, dental, rehabilitation and home health coverage without co-pays. (1) M4A plans are getting enough traction that its potential enactment is “hammering” the value of healthcare stocks. (2)
It’s time for a constructive debate on universal health insurance. The United States is a rich country. The American people deserve access to appropriate and affordable healthcare services. No individual or family should experience financial hardship to pay medical bills.
Unfortunately, M4A as promoted by Sen. Sanders is not a constructive alternative. It is a fiscal train wreck. Medicare’s program design and rate-setting mechanisms are the principal reasons American healthcare costs so much and delivers suboptimal outcomes. More of the same will yield more of the same.
Fortunately, Affordable Health Insurance for All is achievable by harnessing the market’s ability to innovate and create value through sensible payment and regulatory reform. Below the public’s radar, administrators at Health and Human Services (HHS) are currently advancing revolutionary, pro-market reforms. Obama-era administrators who created the Affordable Care Act are supporting them.
It’s time to get real about healthcare transformation. America’s wasteful healthcare system is an embarrassment relative to those operating in other advanced economies. The U.S. spends far more and gets less. By enabling America’s innovation engine to attack healthcare’s inefficiencies, the U.S. can leapfrog centrally managed health systems (like Canada’s) to deliver the right care at the right time in the right place at the right prices.
Political Theater
Today’s main healthcare debate itself, however, is theater of the absurd. On April 15th, tax day, Sen. Sanders participated in a town hall meeting on Fox News (of all places). How ironic, since Sanders and the Fox News audience hold fundamentally opposing views on the role, use and impact of taxes. Sanders pitched M4A to Trump supporters and received an enthusiastic response. (3)
Market socialists like Sanders have never been good at math. Their confidence in the Federal government is completely misplaced. Centralized management of healthcare payment generates over a $1 trillion (an unimaginably large number) in wasteful spending each year.

The marketplace is always smarter than rate-setting central planners. Health companies exploit complex payment formularies for their own benefit at society’s expense. Expanding current Medicare to all Americans would drive up the total annual healthcare costs by tens of billions without expanding preventive care or improving the efficiency of care delivery. M4A would place enormous, unsustainable pressure on the Federal treasury. Both the left-leaning Urban Institute (4) and the right-leaning Mercatus Center (5) agree on this conclusion.
President Trump’s jihad against Obamacare is equally misguided. On March 25th, Trump’s administration’s Justice Department announced that it was supporting Federal Judge Reed O’Connor’s opinion that the Affordable Care Act is unconstitutional. Should the courts uphold O’Connor’s judgment, the ruling will abolish Obamacare in its entirety. (6)
Seemingly unknown to the President, Secretary Alex Azar at HHS is undertaking far-reaching, pro-market reforms to increase price/outcome transparency, facilitate data exchange, lower costs, stimulate innovation and shift financial risk to third parties. Declaring Obamacare unconstitutional would abolish the legal framework for the Trump administration’s progressive payment and regulatory reforms. Talk about the right hand not know what the left is doing.
There is a middle-ground solution between providing “broken” Medicare to everyone and abolishing the ACA. America can achieve universal health insurance coverage at lower costs while fostering consumer choice. This healthcare nirvana combines pluralistic and Affordable Health Insurance for All with meaningful payment and regulatory reform. It delivers better health outcomes, comprehensive preventive care, lower costs, and enhanced community wellness.
Medicare for All’s Fundamental Flaws
Sen. Sanders is an astute politician with a populist bent. He is reaching out to President Trump’s working-class voters with the promise of great healthcare for those who cannot afford or access it. Many are receptive. M4A is good politics, but it’s terrible economics because the legislation creating Medicare contained two fundamental flaws:
- Cost-plus reimbursement (now called fee-for-service or FFS) pays for treatment activity, not treatment outcomes.
- A prohibition against governmental participation in medical decision making.
Together, these provisions require the government (and commercial health insurers by extension) to pay for all “reasonable” treatments whether or not they deliver appropriate care outcomes. This is how healthcare providers and suppliers manufacture artificial demand for their products and services. Basic economics confirms the obvious: when buyers pay for more services, producers provide more services.
This is American healthcare in a nutshell. The best predictor for cardiology procedures in any given market is not demographics, environmental factors or lifestyle behaviors. It is the number of cardiologists practicing in that market. Supply doesn’t create its own demand in well-functioning markets; supply adjusts to intrinsic levels of demand at various price points.
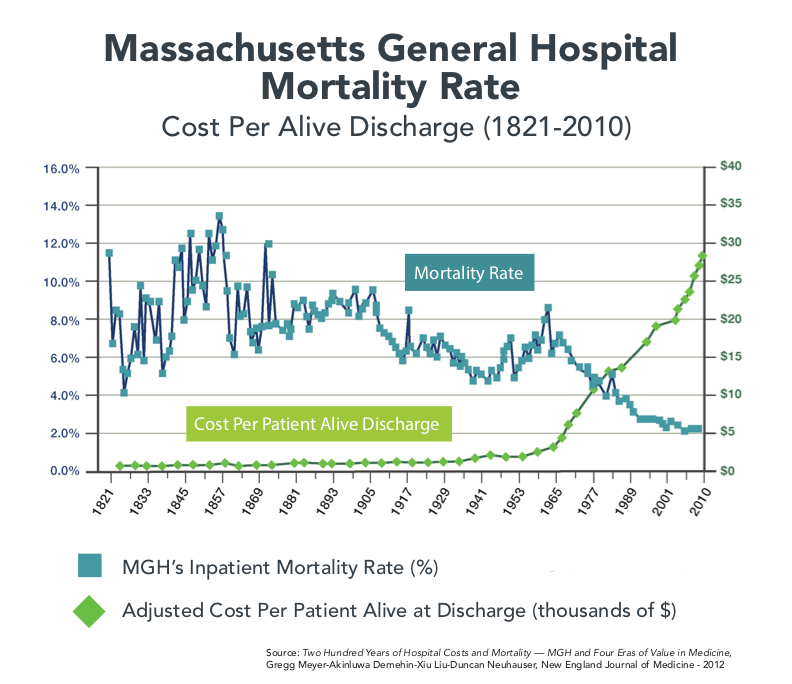
In 2012, The New England Journal of Medicine published an article that examined 200 years of mortality and cost data from Massachusetts General Hospital (MGH). MGH, among the nation’s oldest and most respected hospitals, celebrated its 200th anniversary in 2011.
The data are fascinating. Hospital mortality varied wildly in the 1800s and steadily declined through the 1900s, plateauing at just above 2% in the late 1980s. MGH’s discharge costs go in the opposite direction.
On an inflation-adjusted basis, MGH’s cost per discharge hovered between $1,000 and $2,000 until 1965 and then spiked upward, reaching $30,000 in 2010. What happened in 1965 to trigger this change? Medicare and Medicaid became law.
Supply-driven demand is the reason both the number of procedures and the costs per procedure at MGH and other hospitals have spiraled upward since Medicare’s creation. Fifty-plus years later, America has a bloated acute care delivery system that treats illness and injury at excessive cost but fails to promote health, prevent disease and manage chronic health conditions.
Consequently, job one for policymakers is to normalize healthcare’s supply-demand relationships. Given the right incentives and regulatory environment, health companies will deliver the right care (no over- or undertreatment) at the right time (consumer convenience is essential) in the right facilities (more distributed, less centralized) at the right prices (best outcomes at the lowest costs).
The good news is that healthcare policymakers at HHS understand the challenge and are tackling it with vigor.
Bipartisan Policy Alignment
Given the gulf between President Trump’s and Sen. Sanders’ political positioning on healthcare, a rational observer might expect major differences between HHS officials in the Trump and Obama administrations regarding payment and regulatory reforms. Nothing could be further from the truth.
The irony of the Affordable Care Act is that the ACA was Republican healthcare legislation, but the Democrats passed it without any Republican support. The model for Obamacare was Romneycare in Massachusetts.
Moreover, the ACA’s core features (mandates, public exchanges and insurance supports) originated in conservative think tanks. Without these features, market-based healthcare reform flounders. Republican attempts to “repeal and replace” Obamacare have floundered because they couldn’t configure better market-oriented provisions than those contained in the ACA.
As a consequence, HHS administrators in both the Obama and Trump administrations have embraced value-based care delivery. Foremost on that agenda is replacing fee-for-service payment formularies with programs that shift risk and accountability to third parties.
Pro-market payment reforms include full-risk “bundles” for episodic care and capitated payment models, like Medicare Advantage and HHS’s just announced direct contracting programs for providers (7) for targeted populations. Payment reform alone is not sufficient to correct the system’s fundamental flaws. Consequently, HHS is also promulgating regulatory reforms that promote innovation and level-field competition.
Fixing America’s broken healthcare system is a bipartisan enterprise. For example, there is not a sliver of difference between Adam Boehler, the current Director for the Center of Medicare and Medicaid Innovation, and his Obama-era predecessor Patrick Conway in their determination to rid Medicare of FFS payment.
Boehler proclaimed during a November 2018 interview that “one of our prime goals is to get rid of fee for service [payment].” (8) He’s committed to its complete elimination by 2025. Conway (now CEO of Blue Cross Blue Shield of North Carolina) is equally adamant. At an October 2018 conference, Conway said, “I want fee-for-service, volume-based care to die, and I want to kill it as fast as possible.” (9)
Like Boehler, Conway wants to shift rate-setting responsibilities away from payers to third parties. He even advocates that pre-approved companies bid for select care services, such as colonoscopies and rural Medicare coverage.
During his tenure at CMMI, Conway introduced mandatory bundles for specific procedures. Bundles improve outcomes and drop per unit prices. Boehler is building on Conway’s work to eliminate unnecessary procedures as illustrated by this quote from last November’s interview,
“I don’t know there’s any question that when you have a payment system based on volume, you get exactly that—volume and high prices. So, we’re going to look really at saying, how do you have physicians spend time with their patients and do what they do best and not worry about their revenue cycle but worry about their patients and how you drive outcomes.” (10)
Bohler and Conway are part of a new breed of healthcare buyers who want to use market-based payment models and regulatory reform to eliminate supply-driven incentives for providing excessive healthcare services. Neither objects to providers, payers and suppliers profiting from operating healthcare businesses; however, they want Medicare to “buy health” for its members, not simply high volumes of fragmented medical treatments.
Boehler, Conway and other like-minded reformers want Medicare and other buyers of healthcare services to demand greater value for their healthcare purchases. They want to unleash America’s innovation engine to solve healthcare’s quality, cost and outcome challenges. Health companies that embrace this change will thrive in post-reform healthcare.
Given the right incentives and level-field competition, the marketplace will rationalize care delivery in ways that eliminate overtreatment, undertreatment and overpricing. Consumers will reward companies that deliver coordinated holistic healthcare services that improve individual and community health. In the process, revolutionary upstart and incumbent health companies will deliver the value-based care the American people deserve.
Choice Matters
Medicare for All polls well. Most Americans believe M4A equates to health insurance for all. A January opinion survey (11) by the Kaiser Family Foundation found that 71% of Americans would support M4A if it guaranteed health insurance as a right to all Americans. That support drops to only 37% if M4A eliminates private health insurance (Sen. Sanders’ position) or requires most Americans to pay more taxes.
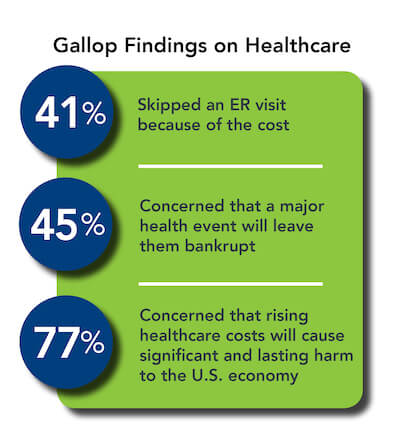
Healthcare confuses and scares most Americans. The following findings from an April 2019 survey (12) by Gallop and West Health reveals that consumer concerns regarding healthcare costs compromise healthcare decision making:
- 45% are concerned that a major health event will leave them bankrupt and 77% are concerned that rising healthcare costs will cause significant and lasting harm to the U.S. economy
- 41% report forgoing a visit to the emergency room due to cost in the past 12 months
- 65 million adults had a health issue but did not seek treatment due to costs in the past 12 months
- Americans borrowed an estimated $88 billion in the past 12 months to pay for healthcare
Paying for healthcare has become an unbearable burden for increasing numbers of Americans. It’s easy to see why many Americans embrace M4A, particularly if it guarantees access to affordable healthcare services. At the same time, 70% of Americans like their health insurance and even more (80%) believe they receive excellent or good healthcare services. (12)
Over 180 million Americans receive health insurance through their employers. It’s ludicrous to believe this mass of Americans, who are largely happy with their healthcare, would universally embrace Medicare for All. Americans want better, more affordable healthcare services, not a government-run, single payer health system.
Further muddying the waters, Americans consume heavily subsidized healthcare services. They rarely pay actual costs. Consequently, Americans have limited understanding of healthcare costs and limited ability to tailor health insurance coverage to their specific preferences.
Those organizations paying for healthcare costs, primarily self-insured employers and governments, design all-encompassing benefit programs for their employees and beneficiaries. As a result, most Americans carry more health insurance than they require, which fuels escalating healthcare expenditures. Self-insured employers pay too much for healthcare because they pay premium prices for excessive coverage that incents treatment activity, not treatment outcomes.
Converting healthcare’s consumers into customers or buyers of health insurance programs is essential to market-driven reform. This already happens when consumers select Medicare Advantage plans or purchase health insurance on public exchanges. These consumers select health insurance plans tailored to their needs. This is where market-based policy reforms, like those advocated by Adam Boehler and Patrick Conway, align with consumer needs.
Helping Americans make better healthcare purchasing decisions will lead to more efficient healthcare delivery. Few empowered consumers would purchase health insurance that pays $5,000 for colonoscopies at academic medical centers when they could receive the identical treatment more conveniently for $500 in a retail setting. The price of that type of health insurance would be too high for the benefits received.
Introducing value into consumers’ healthcare purchasing decisions has a revolutionary impact on the healthcare marketplace. Consumers reward efficient, high quality companies with great customer service. Their wallets do the talking.
Getting Real
When giving talks on market-based healthcare transformation, I often ask audiences to answer the following three yes-or-no questions with a show of hands.
- The U.S. spends 18% of its economy on healthcare. The next big country with the next highest percentage is France at 12%. How many believe the U.S. needs to spend more than 18% of its economy to provide superior healthcare services to everyone in the country? No one ever raises their hand.
- The U.S. spends 75% of its healthcare dollars on chronic disease. How many believe we’re winning the war against chronic disease? No one ever raises their hands.
- On a relative basis, how many believe the U.S. needs to shift resources out of acute and specialty care into health promotion, primary care, chronic disease management and behavioral health? Everybody raises their hands.
What does this short exercise teach? Healthcare doesn’t have a funding problem; it has a resource distribution problem. It’s not tackling the country’s primary healthcare challenge, exploding chronic disease. And the industry needs major restructuring.
There is more than enough funding to provide affordable healthcare to all based on consumer choice and value-driven service provision. Americans don’t need to pay more taxes for universal healthcare coverage, they need to become better buyers of health and healthcare services. By implementing payment reform, customers and private/public payers will demand better outcomes and pay less for getting them.
Affordable Health Insurance for All will improve resource allocation, lower costs and enhance essential primary care services. Efficient healthcare purchasing will liberate funding to pay higher wages and invest in more productive industries.
The gap between political rhetoric on healthcare reform and the operating realities of market-based reforms is profound. Affordable health insurance for all is achievable. Republican and Democrat reformers are taking up the challenge. Draining the emotion from the healthcare political debate and supporting progressive payment and regulatory reform will be essential to their success.
America’s healthcare system will not change the way it delivers care until healthcare buyers change the way they purchase healthcare services. Value must triumph over volume. Entrenched incumbents will not change business models until the marketplace forces them to do so. This requires regulatory reform that creates level-field competition, rewards superior performance and stimulates innovation.
The path forward is clear. Government and the marketplace must align to promote better healthcare purchasing that rewards efficient, high-quality healthcare service provision. Incentives, competition, innovation, rules and enforcement must create a healthcare marketplace where outcomes matter, customers count and value rules.

Sources
- https://www.vox.com/2019/4/10/18304448/bernie-sanders-medicare-for-all
- https://www.nytimes.com/2019/04/19/business/medicare-for-all-health-care-stocks.html
- https://www.cnbc.com/2019/04/16/bernie-sanders-gets-medicare-for-all-support-at-fox-news-town-hall.html
- https://www.urban.org/sites/default/files/publication/80486/200785-The-Sanders-Single-Payer-Health-Care-Plan.pdf
- https://www.wsj.com/articles/even-doubling-taxes-wouldnt-pay-for-medicare-for-all-1533163559
- https://www.nytimes.com/2019/03/25/us/politics/obamacare-unconstitutional-trump-aca.html
- https://www.modernhealthcare.com/payment/cms-launch-new-direct-contracting-pay-models-2020
- https://www.fiercehealthcare.com/payer/cmmi-s-adam-boehler-wants-to-blow-up-fee-for-service
- ibid
- ibid
- https://www.kff.org/health-reform/poll-finding/kff-health-tracking-poll-january-2019/
- https://news.gallup.com/poll/248081/westhealth-gallup-us-healthcare-cost-crisis.aspx
- https://news.gallup.com/poll/245195/americans-rate-healthcare-quite-positively.aspx

About the Author
Recent Posts


